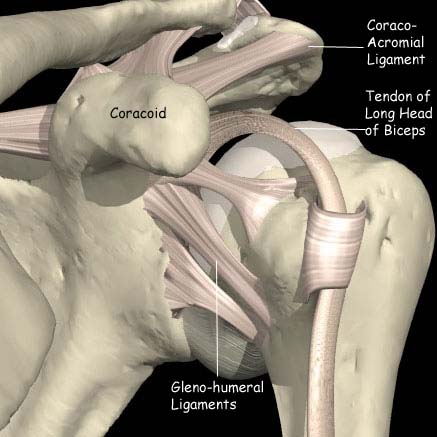
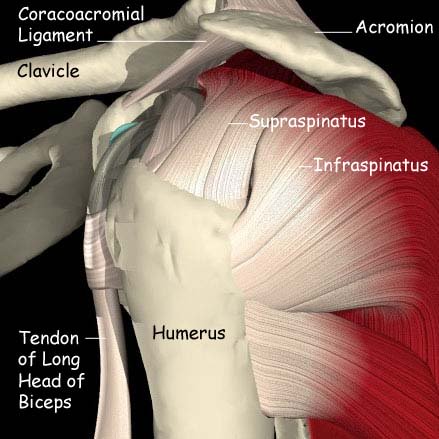
The rotator cuff is comprised of the 4 muscles and tendons that surround the top of the upper arm bone (humerus) and hold it in the shoulder joint. A tear may result suddenly from a single traumatic event or develop gradually. There is often a preceding history of impingement symptoms.
Risk factors
- Degeneration due to aging.
- Subacromial impingement (painful arc)
- Repetitive overhead motion, such as pitching or painting a ceiling.
- Heavy lifting.
- Excessive force, such as a fall.
Signs and symptoms
These are often very similar to subacromial pain syndrome and initially it may be difficult to distinguish between the two.
- Recurrent, constant pain, particularly with overhead activities.
- Pain at night that prevents sleeping on the affected side.
- Muscle weakness, especially when attempting to lift the arm above shoulder height.
- Catching and grating or cracking sounds when the arm is moved.
- Limited motion.
Rotator cuff tears may be partial- or full-thickness. Partial-thickness tears do not completely divide the tendon and may respond well to nonoperative treatments. Full-thickness tears may require surgery to correct if they continue to cause problems (pain or weakness) despite conservative treatment. Surgery may also be used to treat partial-thickness tears that do not respond to nonoperative treatment.
How is the diagnosis made?
The doctor will listen to the description of the symptoms and examine the shoulder for pain and weakness.
Several investigations may be required to confirm the diagnosis, these can include:
- X-Ray
- Ultrasound
- MRI
Treatment options
In most cases, the initial treatment is nonsurgical and involves several modalities.
- Rest. If the tear is due in part to overuse, resting the shoulder may help.
- Physiotherapy to strengthen the muscles, especially those which are not involved are recommended.
- Nonsteroidal anti-inflammatory medications will help control pain.
- Corticosteroid injections can help reduce pain but often do not last very long.
- Suprascapular nerve blocks
There are several surgical options to treat rotator cuff tears, depending on the size, depth, and location of the tear. If other problems with the shoulder are discovered during the surgery, they can be corrected at the same time.
Some tears are not amenable to surgical repair.
The Torbay Rehabilitation Programme for the rotator cuff deficient shoulder developed by Consultant Physiotherapist Dr. Roberta Ainsworth has proved to be very successful in some patients.
Ainsworth Rehabilitation Programme video
Rehabilitation
It takes some time to recover from shoulder surgery. Full function may not return for up to a year. A physiotherapy program of exercises to strengthen and restore motion will be started after surgery. Commitment to following the program outlined will make a difference in the ultimate results. Although every case is unique, surgery can relieve pain for most people and rehabilitation can restore a functional (but often not full) range of motion.