The Condition
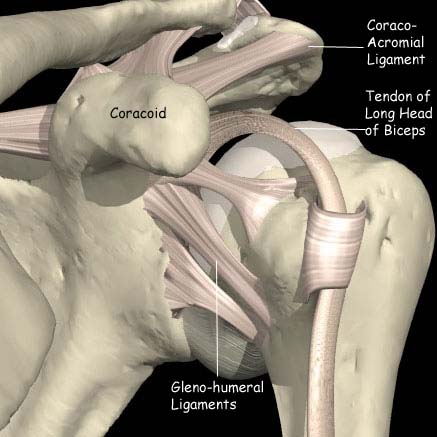
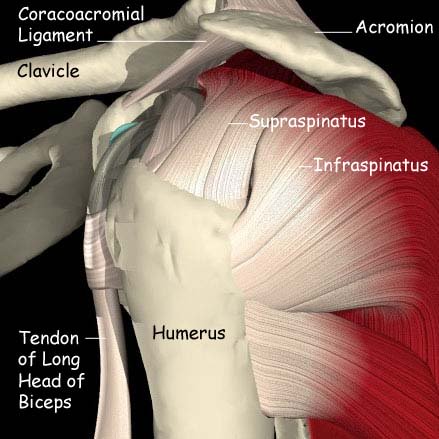
The long head of the biceps tendon ruptures in three groups of patients. Most commonly it is the older patient and may be associated with subacromial impingement or occasionally a rotator cuff tear. Less commonly it is seen in the middle aged patient and is us often associated with a history of weightlifting. In the younger patient rupture of the tendon is occasionally seen with acute forceful injury.
What are the signs and symptoms?
The patient usually complains of a pain in the front of the shoulder followed by a popping feeling. There is then a characteristic deformity seen in the biceps muscle. This is the so called “Popeye” sign in which the muscle belly appears to move towards the elbow as the elbow is flexed. The pre-existing pain often settles rapidly.
In the older patient there is often no residual problem apart from a cosmetic deformity. The younger patient may complain of aching and pulling in the upper arm, particularly as the elbow is flexed.
How is the diagnosis made?
The clinician will take a full history and examine the shoulder and arm. In most cases no further investigation is necessary. Occasionally, if there is concern about the rotator cuff tendons, an MRI may be arranged to assess them.
What is the initial treatment?
The initial treatment is symptomatic and includes rest and anti-inflammatories. In the older patient the discomfort usually settles within a few weeks and there are no residual problems apart from a cosmetic deformity, the “popeye sign”.
Once the acute symptoms have settled down physiotherapy may have a role to improve the shoulder function following injury.
If initial treatment doesn’t work, what’s next?
The younger patients may complain of a persistent ache in the front of the arm, made worse by lifting or carrying.
If the symptoms are intrusive enough then biceps tenodesis may be necessary.