Indications for operation
Irreparable Rotator cuff rupture
Irreparable Rotator cuff rupture
All surgical procedures have some element of risk attached.
The risks outlined below are the most common or most significant that have been reported.
Usually all the pain is removed. Some patients experience mild pain on overhead activities. Rarely is the pain not improved by surgery.
If an infection does occur it is usually superficial in the wounds and is easily treated with antibiotics.
Rarely the infection can be deep inside the joint and this requires surgery to wash the joint out.
The axillary nerve runs close to the bottom of the joint and, if damaged causes weakness of the deltoid muscle and difficulty in raising the arm.
The shoulder will often become stiff after surgery and this usually settles with physiotherapy. Rarely the shoulder can become very stiff and require manipulation or arthroscopic release surgery.
The graft can fail to heal resulting in it “re-tearing”. Failure does not guarantee a poor result, return of pain, or poor function but often does mean a loss of strength.
eo.
General Anaesthetic with an interscalene block (Fully asleep with a local anaesthetic injection into the side of the neck will numb the nerves to the shoulder for post-operative pain relief)
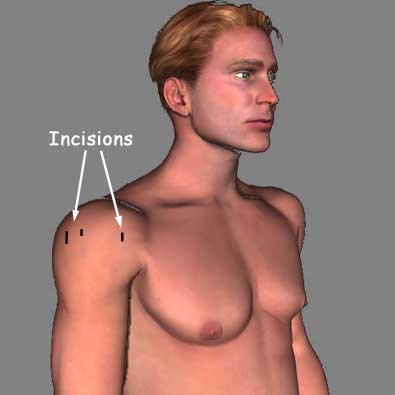
Arthroscopic
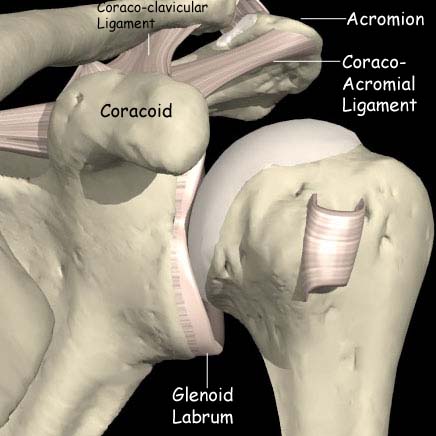
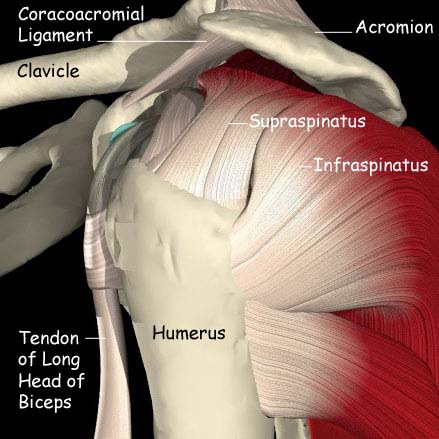
The gleno-humeral (shoulder) joint will be inspected first followed by the subacromial bursa and the rotator cuff. A soft tissue shaving device will be used to clear any scar tissue away. A bone-shaving device will be used to shape the underside of the acromion (the bone at the top of the shoulder) and remove any excess bone.
The edges of the cuff tear are tidied with the soft tissue shaver. The top of the glenoid (socket) and the greater tuberosity (where the cuff normally attaches to the humerus or arm bone) are prepared. Stitches are attached to the bone using small screw type anchors. These stitches are passed through a specially prepared graft which is made of either porcine (pig) or human tissue.
The graft is introduced into the shoulder and the stitches are tied down securing the graft between the socket and the arm. This reproduces some of the function of the native rotator cuff.
Small butterfly paper stitches will be used to close the wounds.
Elastoplast dressings will be placed over the top of the paper stitches and an adhesive bandage over the top of this.
An adhesive dressing will be placed over the wound and the arm will be placed in a sling. You are allowed to take the arm out of the sling to perform basic tasks for 6 weeks before physiotherapy starts. You can go home when you feel comfortable and will be given instructions on what to do next.
Further instructions for Superior Capsule Reconstruction rehabilitation