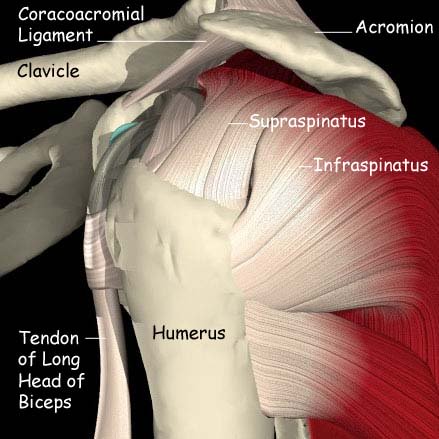
Calcific Tendonitis is a condition in which a small calcium deposit develops in the rotator cuff tendons causing the tissues in the subacromial space to become inflamed causing pain.
It is often difficult to distinguish between calcific tendonitis and subacromial pain however the treatment is the same.
The cause of calcific tendonitis is unknown but it tends to affect those in middle age.

What are the signs and symptoms?
There are two different presentations
1. Acute severe pain. This is usually described by patients as “the worst pain ever”. It comes on over a few hours and the patients will often attend A&E for pain relief. After the acute episode settles the milder form may become a feature.
2. Chronic, repeated episodes of moderate pain which is very similar to subacromial pain syndrome.
This can include
- Mild to severe pain
- Limited movement.
- Inability to hold the arm in certain positions e.g. reading a newspaper
The pain often has two forms
A continuous dull ache, which is often worse at night, is usually located over the lateral aspect of the shoulder joint and may extend someway down the side of the arm even as far as the elbow. Often it does not appear to be coming from the joint at all.
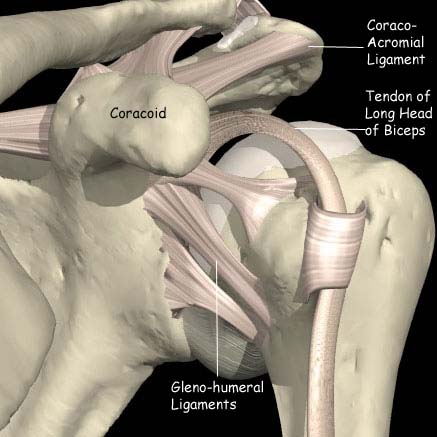
Sharp pain on lifting the arm is felt just below the acromion (the bony prominence at the top of the shoulder). The pain usually starts when the arm reaches horizontal and eases off if the arm can be brought all the way to vertical. This is the so called “painful arc”.
How is the diagnosis made?
The clinician will listen to the description of the symptoms and examine the shoulder. X-rays will be taken to examine the shape of the acromion and to help exclude other pathology within the shoulder. Ultrasound may also be used to identify the calcific deposit.
What is the initial treatment?
In the acute, severe phase a local anaesthetic and steroid injection into the subacromial bursa will produce rapid and lasting relief.
In the more chronic phase then the following the following may be tried.
- Avoidance of the aggravating activities.
- Anti-inflammatory drugs should be used and may be all that is required.
- Local injection of local anaesthetic and steroid often settle the acute episode.
- Ultrasound guided “barbotage” in which the calcium is needled and attempts are made to aspirate the deposit.
- Shockwave Therapy may also be recommended (as is used for Kidney Stones) to break up the deposit
If initial treatment doesn’t work, what’s next?
If the symptoms persist despite conservative treatment the shoulder will be re-examined. It may be necessary to perform an arthroscopic removal of the calcific deposit.